
Glaucoma is a leading cause of irreversible blindness in the U.S., affecting over 4 million people as of 2022. The condition often progresses silently, with no symptoms until significant damage has occurred. Early detection through targeted screenings is critical, especially for high-risk groups.
Key Takeaways:
- Who’s at Risk?
- Adults over 60 (risk increases with age).
- Black and Hispanic populations (higher prevalence and undiagnosed cases).
- Those with a family history, diabetes, or long-term corticosteroid use.
- People with conditions like high myopia, thin corneas, or obstructive sleep apnea.
- Screening Tests:
- Eye pressure measurement (tonometry).
- Visual field testing for peripheral vision loss.
- Imaging (OCT) to detect optic nerve damage early.
- Gonioscopy to evaluate drainage angles.
- Corneal thickness measurement (pachymetry).
- How Often?
- Baseline exam at age 40.
- Screenings every 1–2 years for high-risk individuals.
- Annual exams covered by Medicare for eligible high-risk groups.
Glaucoma screenings save vision by identifying damage before symptoms appear. If you’re at risk, schedule a dilated eye exam today.
Ask An Expert: Glaucoma Risk Factors, Symptoms, and Future Research
sbb-itb-246add9
Glaucoma and Its Impact on Vision Health
Glaucoma Risk by Demographics & Screening Guidelines
What Is Glaucoma?
Glaucoma refers to a group of progressive eye disorders that harm the optic nerve, the vital connection between your eyes and brain. When this nerve is damaged, your field of vision gradually shrinks, and unfortunately, the damage is permanent.
In the U.S., the most prevalent type is Primary Open-Angle Glaucoma (POAG), making up about 75% of cases. In POAG, the drainage angle of the eye stays open, but fluid fails to drain properly, leading to a slow and painless increase in pressure. This gradual progression often means people don’t realize there’s an issue until they’ve already lost a significant portion of their vision.
Another form, Angle-Closure Glaucoma (ACG), presents differently. Here, the iris blocks the drainage angle, which can result in a sudden onset of severe eye pain, nausea, blurred vision, and rapid vision loss. Immediate medical attention is critical for this type. Lastly, there’s Normal-Tension Glaucoma, where optic nerve damage occurs even when eye pressure is within the normal range (below 21 mm Hg).
Understanding these types is key to grasping the broader impact of glaucoma on vision health in the U.S.
How Common Is Glaucoma in the U.S.?
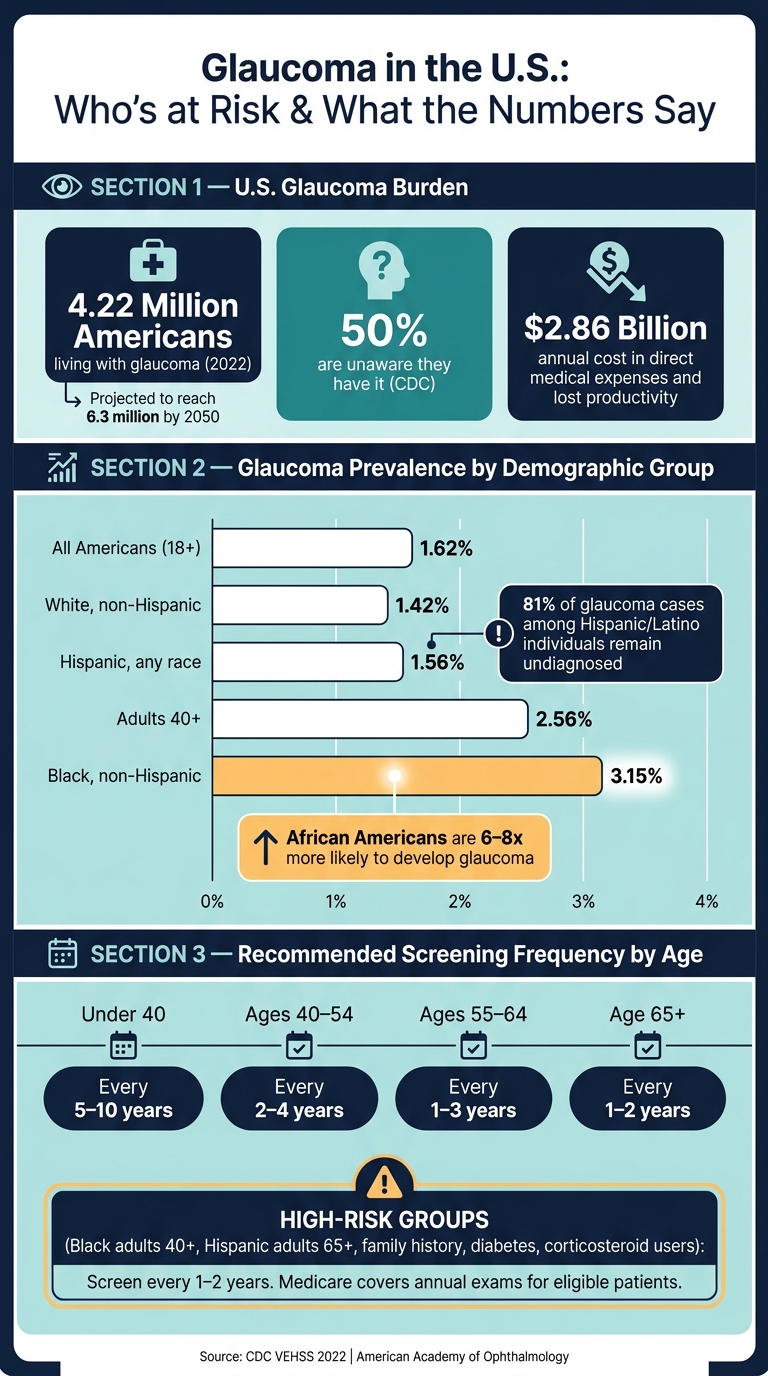
As of 2022, approximately 4.22 million Americans were living with glaucoma, with about 1.5 million experiencing vision impairment as a result. By 2050, that number is expected to climb to 6.3 million, driven by an aging population and changing demographics.
One of the most alarming aspects of glaucoma is how often it goes undetected.
"Because there are usually no symptoms, only 50% of people with glaucoma even know they have it." – CDC
The problem is even more pronounced in certain groups. A 2016 study revealed that 81% of glaucoma cases among Hispanic or Latino individuals remain undiagnosed, compared to 73% among non-Hispanic White individuals. Additionally, Black non-Hispanic adults face a glaucoma prevalence rate of 3.15%, more than double the 1.42% seen in White non-Hispanic adults.
The economic impact is also significant, with glaucoma costing the U.S. around $2.86 billion annually in direct medical expenses and lost productivity.
| Demographic Group | Glaucoma Prevalence | Vision-Affecting Glaucoma |
|---|---|---|
| All Americans (18+) | 1.62% | 0.57% |
| Black, non-Hispanic | 3.15% | 0.74% |
| White, non-Hispanic | 1.42% | 0.47% |
| Hispanic, any race | 1.56% | 0.25% |
| Adults 40+ | 2.56% | 0.91% |
Source: CDC VEHSS 2022 Modeled Estimates
These statistics highlight an important reality: glaucoma doesn’t affect all groups equally. Some populations face a much higher burden, and without regular screenings, many people will only discover the disease after irreversible vision loss has occurred.
Who Is at High Risk for Glaucoma?
Glaucoma doesn’t affect everyone the same way. Some people develop it earlier, and for others, it progresses more aggressively. Knowing who is most at risk can help protect your vision.
How Age Affects Glaucoma Risk
The likelihood of developing glaucoma increases significantly as you age. For example, its prevalence jumps from 2.14% in people aged 60–64 to over 8% for those aged 85–89. In fact, adults over 60 are six times more likely to develop glaucoma. Because of this, the American Academy of Ophthalmology advises getting a baseline eye exam at age 40, with more frequent checkups as you grow older and risk factors accumulate.
Racial and Ethnic Risk Factors
Certain racial and ethnic groups are more prone to glaucoma. For instance, African Americans are 6–8 times more likely to develop the disease. Glaucoma is also a leading cause of blindness among Black and Latinx populations, with Hispanic individuals experiencing higher risks after age 60. Meanwhile, people of Asian descent, especially those of Japanese heritage, face a greater likelihood of developing normal-tension and angle-closure glaucoma. In fact, over 75% of global cases of acute and chronic angle-closure glaucoma occur in individuals of Asian descent. To address these disparities, Medicare covers annual glaucoma screenings for Black adults aged 50 and older, as well as Hispanic adults aged 65 and older.
Family History and Related Medical Conditions
Having a family history of glaucoma significantly raises your odds – by 4 to 9 times – and siblings of those with glaucoma are up to 10 times more likely to develop it themselves.
"One of the biggest risk factors for glaucoma is if it runs in your family. So, if you have a first-degree blood relative with glaucoma, you should definitely get your eyes checked." – Daniel Petkovsek, MD, Glaucoma Specialist
Beyond genetics, several health conditions and eye characteristics can increase your risk:
| Risk Factor | Why It Matters |
|---|---|
| Diabetes (Type 2) | Raises the risk of primary open-angle glaucoma (POAG) and can lead to secondary neovascular glaucoma. |
| Hypertension/Hypotension | Affects blood flow and pressure to the optic nerve. |
| High Myopia (Nearsightedness) | Structural changes in the eye make the optic nerve more vulnerable; risk increases by about 20% per diopter. |
| Thin Central Cornea | A strong predictor of glaucoma progression. |
| Long-Term Corticosteroid Use | Associated with a 40% increase in ocular hypertension and POAG, especially with high-dose steroid inhalers. |
| Obstructive Sleep Apnea (OSA) | Linked to POAG, likely due to vascular and oxygen-related issues. |
If you’re using corticosteroids regularly – whether as inhalers, eye drops, or oral medications – it’s crucial to monitor your intraocular pressure (IOP) frequently. Elevated IOP is one of the main drivers of optic nerve damage.
For those at higher risk, scheduling a comprehensive eye exam is essential. At Cheyenne Eye Clinic and Surgery Center, a team of skilled ophthalmologists and optometrists can help with early detection and effective management of glaucoma. Identifying these risk factors is the first step toward timely screening and diagnosis.
Glaucoma Screening Tests You Should Know About
Once you’re familiar with your risk factors, the next step is understanding what happens during a glaucoma screening. A comprehensive eye exam is the best way to catch glaucoma early, relying on several specialized tests. These procedures lay the groundwork for early detection and help guide the diagnostic process.
What Happens During a Full Eye Exam
A thorough glaucoma screening includes five key components: measuring intraocular pressure, evaluating the optic nerve, testing your visual field, assessing the drainage angle (gonioscopy), and measuring corneal thickness. Additionally, a baseline visual acuity and pupil exam are performed. Since central vision is often the last area affected by glaucoma, tracking changes over time becomes easier. A mid-dilated, unresponsive pupil can also signal an acute angle-closure glaucoma crisis.
Intraocular Pressure Measurement and Visual Field Testing
Tonometry measures the pressure inside your eye, known as intraocular pressure (IOP). Goldmann applanation tonometry is the standard method, using contact with the eye’s surface to obtain accurate readings. However, tonometry alone has a sensitivity of 0.48 for detecting glaucoma. It’s worth noting that about one-third of glaucoma cases involve normal-tension glaucoma, where IOP stays below 21 mmHg despite optic nerve damage.
Visual field testing, often done with a Humphrey Visual Field Analyzer, maps your peripheral vision by having you respond to flashes of light. This test has a sensitivity of 0.87 and a specificity of 0.82. Since visual field defects typically don’t appear until about 50% of retinal ganglion cells are lost, repeated tests are often necessary before confirming a diagnosis.
In addition to these tests, advanced imaging plays a critical role in refining the diagnosis.
Imaging and Specialized Diagnostic Tests
Optical Coherence Tomography (OCT) uses infrared light to create detailed cross-sectional images of the retina and optic nerve head. This test can detect thinning in the retinal nerve fiber layer even before any noticeable vision loss occurs. Spectral domain-OCT offers a sensitivity of 0.79 and a specificity of 0.92 for identifying glaucoma.
Two other tests complete the evaluation. Pachymetry measures corneal thickness, which is important because thinner corneas are linked to a higher risk of glaucoma and can lead to underestimated IOP readings. Gonioscopy, on the other hand, uses a special lens and slit lamp to examine the drainage angle, helping to distinguish between open-angle and angle-closure glaucoma. Dr. Douglas J. Rhee from University Hospitals/Case Western Reserve University highlights:
"Thinning of the neurosensory rim (optic nerve or retinal nerve fiber layer) over time alone can be diagnostic of glaucoma regardless of the IOP or visual field."
| Test | What It Evaluates | Why It Matters |
|---|---|---|
| Tonometry | Intraocular pressure (IOP) | High pressure is the main modifiable risk factor |
| Ophthalmoscopy | Optic nerve head | Identifies "cupping" or nerve fiber damage |
| Visual Field Testing | Peripheral vision | Detects functional loss that might go unnoticed |
| OCT Imaging | Retinal nerve fiber layer | Detects structural damage before vision loss |
| Gonioscopy | Drainage angle | Differentiates open-angle from angle-closure glaucoma |
| Pachymetry | Corneal thickness | Improves IOP accuracy and identifies additional risk |
At Cheyenne Eye Clinic and Surgery Center, we include all these advanced tests in our comprehensive eye exams to ensure early detection and proper management of glaucoma.
How Often Should High-Risk Groups Get Screened?
The frequency of eye screenings depends on individual circumstances, including age, personal risk factors, and whether any early warning signs have been detected.
General Screening Guidelines for Adults
The American Academy of Ophthalmology suggests that all adults, even those without symptoms or known risk factors, get a baseline comprehensive dilated eye exam at age 40. After this initial check, follow-up schedules depend on the findings and individual risk factors. For adults with no heightened risk, the recommended intervals are as follows:
| Age Group | Recommended Screening Interval |
|---|---|
| Under 40 | Every 5–10 years |
| Ages 40–54 | Every 2–4 years |
| Ages 55–64 | Every 1–3 years |
| Age 65 and older | Every 1–2 years |
It’s important to note that a dilated eye exam is crucial – simple pressure checks aren’t enough. These general guidelines provide a baseline, but high-risk individuals require more frequent evaluations.
Screening Frequency for High-Risk Groups
For those at higher risk, screenings should occur every 1–2 years. This includes Black/African Americans aged 40 and older, all adults over 60 (with a particular focus on Mexican Americans), and anyone with a family history of glaucoma. Regular screenings are also essential for individuals with diabetes, obstructive sleep apnea, or a history of prolonged corticosteroid use.
The financial burden of frequent screenings can be a concern, but Medicare and Medicaid offer annual coverage for glaucoma exams for eligible high-risk patients, including those with diabetes or a family history of the disease. This support makes it easier for patients to maintain their screening schedules.
Monitoring Glaucoma Suspects and Diagnosed Patients
For individuals identified as glaucoma suspects – those with elevated eye pressure or optic nerves that appear suspicious but show no confirmed damage – regular follow-ups replace periodic screenings. These follow-ups typically occur every 6 to 12 months and involve tests like OCT imaging, visual field assessments, and tonometry to track structural or functional changes.
Because glaucoma often progresses silently, sticking to a regular monitoring schedule is key. Even if you feel fine, staying consistent with follow-ups can make a significant difference in preserving your vision. At Cheyenne Eye Clinic and Surgery Center, we collaborate with each patient to create a personalized plan tailored to their risk factors and needs.
Conclusion
Glaucoma often progresses without warning, and by the time symptoms appear, the damage to vision is usually permanent. This is why early screening is so important, especially for those at higher risk.
In the United States, about 50% of the 4 million people with glaucoma are unaware they have it. For Black and Hispanic populations, glaucoma is the leading cause of irreversible blindness. Additionally, individuals over 60 are six times more likely to develop this condition compared to younger adults. These figures highlight how early intervention can make a difference in preserving sight.
"Early detection and timely treatment with medication or surgery can arrest further vision loss and prevent blindness. While the destructive path of glaucoma can be halted or slowed, its deleterious effects cannot be reversed." – Karen Allison, MD
Early detection hinges on advanced, comprehensive evaluations. At Cheyenne Eye Clinic and Surgery Center, cutting-edge diagnostic tools like OCT, visual field analysis, gonioscopy, and pachymetry help identify subtle changes before vision loss occurs. Individualized care plans are crafted based on each patient’s unique risk factors, whether that involves closer monitoring, setting a target intraocular pressure (IOP), or exploring treatment options such as Selective Laser Trabeculoplasty (SLT).
Taking a proactive approach is essential to preventing irreversible vision loss. If you fall into a high-risk category, schedule a comprehensive dilated eye exam as soon as possible. At Cheyenne Eye Clinic and Surgery Center, the focus is on personalized glaucoma screening and care – because protecting your vision begins with understanding your risks.
FAQs
Can you have glaucoma with normal eye pressure?
Yes, you can develop glaucoma even if your eye pressure is within the normal range. This condition is known as normal-tension glaucoma or low-tension glaucoma. In this type, the optic nerve sustains damage despite having pressure levels that fall within the typical range. Because eye pressure alone doesn’t provide the full picture, a thorough eye exam is essential. This includes an evaluation of the optic nerve and visual field testing. For those at higher risk, regular screenings are especially important to catch this condition early.
What’s the difference between an eye pressure check and a full glaucoma screening?
Tonometry, or an eye pressure check, measures the fluid pressure inside your eye. However, it’s not enough to diagnose glaucoma by itself. A complete glaucoma screening goes further, including a dilated eye exam, an evaluation of the optic nerve, an assessment of the drainage angle, and peripheral vision tests. These additional steps can uncover glaucoma even when eye pressure appears normal or reveal damage that tonometry might overlook.
If my results are borderline, what happens next?
If your screening results indicate borderline findings or suggest you might be a glaucoma suspect, your eye care provider will conduct a thorough evaluation to confirm the diagnosis or decide if treatment or monitoring is necessary. This process may involve several tests, including a dilated eye exam, gonioscopy, pachymetry, visual field testing, and advanced imaging techniques like OCT (optical coherence tomography). Cheyenne Eye Clinic and Surgery Center offers these detailed diagnostic services to ensure precise assessments and effective follow-up care.